A 55 year old female with fever,neck stiffness and headache.
This is online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable inputs on comment box is welcome.


A 55 YR OLD FEMALE WITH FEVER , NECK STIFFNESS AND HEADACHE.
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
Hall ticket number:1701006168.
Final practical exam long case.
CHIEF COMPLAINTS:
A 55 year old female, house wife by occupation came with chief complaints of
Fever since 5 days.
Neck stiffness since 5 days.
HISTORY OF PRESENTING ILLNESS:
-Patient was apparently asymptomatic 5 days back then she had fever which is sudden in onset and continuous type and relieved on medication.
-Complaints of bilateral knee joint pains
-Fever not associated with chills and rigors. No h/o cold ,cough ,loose stools , abdominal pain , breathlessness, PND , orthopnoea. No history of burning micturition, increased frequency of micturition.
-There is h/o headache from 25 days but it got aggravated since 5 days which is insidious in onset and progressive and not relieved on medication, No aggravating and relieving factors .
- History of neck stiffness since 5 days.
-History of vomiting 3 days back ,1 episode which is not projectile ,non bilious ,content is food particles .
Past history:-
No history of similar complaints in the past.
Medical illness - Not a known case of diabetes , hypertension, asthma, TB, Thyroid .
•7 yrs back she had history of CVA where both upper and lower limbs are paralysed and took some medication.
she took allopathy medicine 6 months back and she got recovered.
•Surgical history- hysterectomy done 25 yrs back .
Family history:-
No similar complaints inthe family
No history of diabetes, hypertension,TB ,asthma.
Personal history:-
Diet - mixed
Appetite - lost
Sleep - adequate
Bowel and bladder- regular bladder and constipation is present .
No addictions and allergies.
General examination:-
Patient is conscious, coherent, coperative. Moderately built moderately nourished.
No pallor, icterus, cyanosis, clubbing, generalised lymphadenopathy, generalised edema.
Vitals:
Temperature: 99°F
Pulse rate: 75bpm
Resp rate:15cpm
BP:110/70mmhg
Spo2:96%.
Systemic examination:-
Central nervous system-
Higher mental functions
• conscious
• oriented to person and place ,time.
• memory - able to recognize their family members
• Speech - normal.
Cranial nerve examination -
• 1 - sense of smell present
• 2- Direct and indirect light reflex present
• 3,4,6 - no ptosis Or nystagmus
• 5- corneal reflex present on both sides
• 7- no deviation of mouth, no loss of nasolabial folds, forehead wrinkling present.
• 8- able to hear
• 9,10- uvula not deviated
• 11- sternocleidomastoid contraction present
• 12- no tongue deviation.
Motor system
Tone -. Upper limbs Lower limbs
Inspection - Normal Normal
Palpation - Normal Normal
Bulk : right Left
Arm 28cm 27cm
Forearm 20cm 18 cm
Thigh 33 cm 32cm
Calf 25 cm 23 cm.
Power :
Muscles of neck -
• stenocleidomastoid- good
•Nuchal muscles- stiffness present
Slight tenderness present over the neck on examination.
Right Left
Biceps- 5/5 5/5
Triceps-. 5/5 5/5
Brachioradialis-. 5/5 5/5
Tibialis posterior-. 5/5 5/5.
Reflexes: right left
Biceps- + +
Triceps- + +
Supinator- + +
Knee- + +
Ankle - + +
Sensory system: Normal
Cerebellar signs :
Knee - heel incoordination - No
Finger - nose incoordination- No
Meningeal signs -
Neck stiffness present .
Kernig's sign - positive
Brudzinki sign - positive.
EXAMINATION OF OTHER SYSTEMS
CARDIOVASCULAR SYSTEM:
S1 S2 Heart sounds – normal
No thrills/murmurs
RESPIRATORY SYSTEM:
Chest symmetrical, No paradoxical movements, Normal vesicular breath sounds heard,
No abnormal/added sound
ABDOMEN:
Abdomen is soft, non tender,No organomegaly, No ascites.
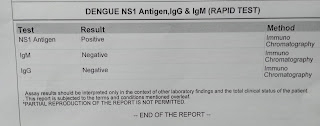
Provisional diagnosis:-
Dengue fever with viral meningo encephalitis under evaluation and detected denovo diabetes mellitus type 2.
Investigations:-
GRBS - 91 mg/dl
Hemogram :-
Hb - 13 g/dl
TLC - 3500
N/L/E/M-60/30/2/8
PLT- 2.1 lakh per mm3
NC/NC
Fasting blood sugar- 168 mg/ dl
Hb1 AC -6.9
Urea- 38
Serum creatinine- 1.0
Uric acid - 4.9
Sodium- 141meq
Pottasium- 4.0
chloride- 105.
Serology - non reactive
LFT:
Tb - 1.03
Db- 0.31
SGOT(AST) - 69
SGPT(ALT) - 68
ALP-135
Tp-6.4
Albumin-4.0
CUE:
Albumin +
Sugar - nil
Pus cells - 6 - 8
Epithelial cells- 3-4
RBC - nil
Casts - nil .
CSF :
Sugar - 81
Protein-12.6
Chloride-113
ABG:
pH - 7.4
Pco2- 29.1
Po2- 88.4
Hco3- 18.0
Sat O2 - 96%.






Treatment:-
Inj. CEFTRIAXONE 2 gm/ BD
Inj.DEXA 6mg/iv/tid
Inj . Vancomycin 1gm/iv
Inj. Pcm 1gm/iv
Tab . Pcm 650 mg
Tab. Ecospirin 75 mg /po/od
Tab. Atorvas 10 mg /po/od
Syp. Cremaffin plus 30ml/po
On day 2 :-
Patient is conscious, coherent, cooperative.
Vitals:-
Temperature: 99°F
Pulse rate: 76bpm
Resp rate:15cpm
BP:130/90mmhg
Spo2:96%
GRBS- 197mg/dl.
Treatment-
Inj. CEFTRIAXONE 2 gm/ BD
Inj.DEXA 6mg/iv/tid
Inj . Vancomycin 1gm/iv
Inj. Pcm 1gm/iv
Tab . Pcm 650 mg
Tab. Ecospirin 75 mg /po/od
Tab. Atorvas 10 mg /po/od
Syp. Cremaffin plus 30ml/po
Oint.Diclofenac for thigh pain.
On day 3:-
Patient is conscious, coherent, cooperative.
Vitals:-
Temperature: 99°F
Pulse rate: 78bpm
Resp rate:16cpm
BP:120/90mmhg
Spo2:96%
GRBS- 190mg/dl
Treatment-
Inj. CEFTRIAXONE 2 gm/ BD
Inj.DEXA 6mg/iv/tid
Inj . Vancomycin 1gm/iv
Inj. Pcm 1gm/iv
Tab . Pcm 650 mg
Tab. Ecospirin 75 mg /po/od
Tab. Atorvas 10 mg /po/od
Syp. Cremaffin plus 30ml/po
Oint.Diclofenac for thigh pain
Inj.pan 40 mg iv /od
Tab. Naproxen 250 mg po/tid.
Flexbenz gel for L/A on thighs.
Day 4:
Inj. CEFTRIAXONE 2 gm/ BD
Inj.DEXA 6mg/iv/tid
Inj . Vancomycin 1gm/iv
Inj. Pcm 1gm/iv
Tab . Pcm 650 mg
Tab. Ecospirin 75 mg /po/od
Tab. Atorvas 10 mg /po/od
Syp. Cremaffin plus 30ml/po
Oint.Diclofenac for thigh pain
Inj.pan 40 mg iv /od
Tab. Naproxen 250 mg po/tid.
Flexbenz gel for L/A on thighs.
Tab metformin 500mg/od.
