57 YEAR OLD WAS PRESENTED RO OPD WITH YELLOW ISH DISCOLORATION OF SKIN,CONJUNTIVA, ABDOMINAL PAIN.
This is an online e log book to discuss our patient health data shared after taking his/her/guardians singned informed consent. Here we discuss our individual patients problems with an aim to solve the patient’s clinical problem with collective current best evident based input.
This E blog also reflects my patient cantered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of “patient clinical data analysis” to develop my competency in reading and comprehending clinical data including history, clinical findings,investigations and come up with diagnosis and treatment plan.
This is a case of 57 year old female , housewife staying in Mathavanga , West Bengal.
CHIEF COMPLAINTS:
- pain in abdomen( since 3 1/2 months {mild} , 2months {progressed} )
- tingling pain in the abdomen , sudden in onset. (increased on eating )
- can't stand / sit without support (since 1month)
- iching all over the body (since 1month)
- generalized weakness
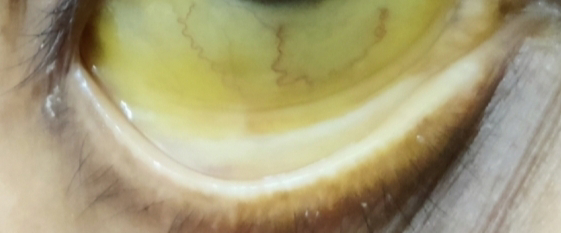
- yellowish discoloration of sclera and skin and stools ( since 25 days ).
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 2months back then she noticed yellowish discoloration of eyes and urine and went to hospital and on further evaluation she was diagnosed to have type 2 diabetes mellitus and was started tab.dapgliflozin 10mg in the morning and tab.sitagaliptin 50mg + t.metformin 500mg at night.
C/o pain over the periumbilical region since 2months ,pricking type of pain ,non radiating,no aggrevating and relieving factors.(slight Decrease in pain from last 2days
H/o occasional tingling and numbness of upper limb and lower limb.
No c/o polyphagia,polydypsia,nocturia.
Past history -
In 1996 diagnosed to have tumour of the uterus ( hysterectomy done)
In 2010, she had difficulty in breathing during winter season and monsoons (? Bronchial Asthma ) and used tab.deriphylline 450mg 1/2 tab PO/BD for 5-7days during the attacks along with inhaler ,presently she is not having any difficulty and not using.
K/c/o diabetes mellitus 2months and on tab.dapgliflozin 10mg in the morning and tab.sitagaliptin 50mg + t.metformin 500mg at night.
Dietary history -
She consumes
tea along chapathi in the morning
Sometimes chole (boiled and mashed )
Afternoon - rice and dal along with some vegetables.
In between biscuits as snacks
And chapathi at night.
Normal - appetite
Adequate -sleep
Regular bowl movements
Normal bladder movements
No history of alcohol, smoking and chewing of tobacco .
FAMILY HISTORY:
No significant family history.
General examination:
Patient is conscious, coherent and cooperative.
No lymphadenopathy, clubbing, koilonychia, clubbing.
Pallor present.
Icterus: present
No clubbing, cyanosis, lymphadenopathy,odema.
Vitals -
Bp - 110/70mm hg
Pr - 86bpm
Rr-16cpm
Grbs -162mg/dl
SYSTEMIC EXAMINATION:
CVS:
S1 and S2 heard.
No addded thrills or murmurs heard
RESPIRATORY SYSTEM:
Normal vesicular breath sounds heard.
Bilateral air entry present.
ABDOMEN:
INSPECTION:
shape of abdomen - schaphoid.
umbilicus -central
no sinuses
No scars
PALPATION:
Tenderness+ over right hypochondriac region


PERCUSSION:
No shifting dullness
AUSCULTATION:
Bowel sounds +
CNS:
Conscious and coherent.
Normal sensory and motor responses
Her recent reports -3/7/23
FBS -102mg/dl
Plbs -190mg/dl
Hba1c - 12.4
FAMILY HISTORY:
No significant family history.
INVESTIGATIONS:
21/7/23








Chest X RAY:
ECG:

2D echo:

Treatment:
1.TAB ZOFER 4 MG PO/BD
2.TAB PAN 40 MG PO/OD BFF
26/07/2023 .
3. TAB. DAPAGLIFOZIN 10mg PO/OD
4. TAB SITAGLIPTIN 50 MG +TAB METFORMIN 500 MB PO/TOD .
4. GRBS MONITORING.
22/7/23:
Surgery refferal was taken I/v/o
Pain in abdomen since 2 months, yellowish discoloration since 2 months, itching all over body since 2 weeks
After examining patient they adviced for ERCP for pancreatic duct stenting with or without biopsy and to continue same treatment.
23/7/23:
Patient complaints of periumblical region pain and generalised pruritis due to which she's having difficulty in sleeping .
Tab ultracet 1/2 tab qid
And t.cetrizine po/bd have been added.
On 24/7/23
Patient was done to KHL for gastro opinion and was adviced for ERCP along with CBD stenting ,if possible biopsy from head of pancreas .
Procedure was done.
S/P: ERCP+ CBD STENTING DONE.
Biliary brushings were taken.


Grbs trends yesterday 25/07/23
7am -236mg/dl
9am - 243mg/dl
12pm -233mg/dl
7pm -181mg/dl
9pm -223mg/dl
26/7/23:
patient c/o pain in the umbilical and right hypochondriac region since yesterday night,with tenderness present in umbilical and right hypochondriac region,no guarding and no rigidity.
Surgery referral was taken.
After examining the patient,they advised
1.Inj magnex forte 1.5 mg IV/BD
2.Inj pcm 1gm IV/BD
3.Inj buscopan IM/STAT
Surgical oncology opinion was taken on 26/7/23 has adviced to wait for cytology reports and repeat lft after 2 weeks to know the status of decompression and if the lft is improved and based on cytology report decision of surgery will be taken(whipples procedure).
and has adviced cect abdomen triple phase with pancreatic protocol to know if the mass is operable or not and location of mass(pancreatic head or mid CBD as reported in ercp) and previous cect films were of poor contrast.
27/7/23:
Patient complaints of pain in peri umbilical and hypochondriac region.
No stools passed since two days.
Nauseating feeling on intake of food.
Had 1 episode of vomiting yesterday late afternoon after eating mango.
Food contents expelled.
P/A: Tenderness around peri umbilicals area and right hypochondrium.
Treatment:
1. Inj. Magnex forte 1.5mg IV/BD
2. Tab.zofer 4mg po/od.
3.Tab.glimiperide 0.5mg po/od in the morning before breakfast
4.Tab.Ultracet 1/2 tab po/qid
5. GRBS monitoring.
Grbs trends:
26/7/23
9am:157mg/dl
11am:145mg/dl
1pm:122mg/dl
6pm:125mg/dl
7pm:128mg/dl
8pm:105mg/dl
10pm:186mg/dl
27/07/23
7am:100mg/dl
8am:110mg/dl
10am:100mg/dl
1pm:87mg/dl
3pm:70mg/dl
8pm:80mg/dl
10 pm:186mg/dl
28/7/23
7am:110 mg/dl
9am:76mg/dl
11am:74mg/dl
1pm:54mg/dl
3pm:50mg/dl
6PM:54 mg/dl
10 PM:59 mg/dl
29/7/23:
7AM:67 mg/dl
Patient complaints of not passing stools since yesterday evening,proctolytic enema was given at 7:30 pm.
29/7/23:
Gastroreferral taken today as advised for follow up after 5days by khl gastroenterologist they adviced USG abdomen and LFT.


30/7/23:
BP-130/70mmhg
PR-80bpm
RR-16cpm
Temp- Afebrile
Patient had 2 episode of loose stools (watery)
She is complaining of boating,nausea.
31/7/2023:
patient complaints of nausea and pain in right hypochondrium.
Treatment:
1.Tab Zofer 4 mg PO/TID
2.Tab ultracet 1/2 tab PO/QID
3.TAB Avil 25 mg PO/QID
4.TAB Pan 40 MG PO/OD
5.GRBS monitoring
GRBS trends:
29/7/23:
8AM:67 mg/dl
10 AM:105 mg/dl
1 PM:119 mg/dl
5 PM:115 mg/dl
10 PM: 59 mg/dl
30/7/23:
7 AM: 48 mg/ dl
10 AM: 80 mg/ dl
1 PM: 95 mg/dl
3 PM:133 mg/dl
6 PM:100 mgldl
8 PM: 122 mg/ dl
1/8/2023:
patient complaints of pain in umbilical region and right hypochondriac region
Vitals:
BP: 100/60 mmhg
PR:78 BPM
RR: 15 cpm
Temperature:97.2 F
Treatment:
1.Tab Zofer 4 mg PO/TID
2.Tab ultracet 1/2 tab PO/QID
3.TAB Avil 2 mg PO/QID
4.TAB Pan 40 MG PO/OD
5.GRBS monitoring
31/7/23:
8 am : 89 mg/dl
10 am:88 mg/dl
1pm:113 mg/dl
4pm:121 mg/dl
7 pm: 100 mg/dl
10 pm:110 mg/ dl
1/8/23:
7 am: 95 mg/dl
3/8/23:
Patient has been taken to khl for EUS and FNAB.



4/8/2023:
patient feels better and abdominal pain - decreased
Vitals:
BP: 120/80 mmhg
PR:80 BPM
RR: 15 cpm
Temperature:97.2 F
GRBS:173 mg/dl
Treatment:
1.Tab Zofer 4 mg PO/TID
2.Tab ultracet 1/2 tab PO/QID
3.TAB Avil 2 mg PO/QID
4.TAB Pan 40 MG PO/OD
5.GRBS monitoring
5/8/23:
patients complaint of generalised pruritis has not decreased and due to which she has not been able sleep yesterday.
Vitals:
BP: 120/60 mmhg
PR:78 BPM
RR: 16 cpm
1.Tab Zofer 4 mg PO/TID
2.Tab ultracet 1/2 tab PO/QID
3.TAB Avil 2 mg PO/QID
4.TAB Pan 40 MG PO/OD
5.GRBS monitoring
GRBS TRENDS:
8AM- 173 MG/DL
4PM- 168 MG/DL
8PM- 145MG/DL
8AM- 97MG/DL
Derma refferal was taken I/v/o pruitits and has been advised to take
1.VENUSIA MAX LOTION FOR LA/BD/2 weeks.
6/7/23:
Patient attender is worried that the patient health is deteriorating from the time of admission
She was actively walking 2 weeks ago but now the patient is weak and not taking food properly
patient complaints of lack of appetite , stools not passed since yesterday.
Vitals:
BP: 120/70 mmhg
PR:80 BPM
RR: 16 cpm
Treatment:
1.Tab Zofer 4 mg PO/TID
2.Tab ultracet 1/2 tab PO/QID
3.TAB Avil 25mg 1/2 tab PO/QID
4. VENUSIA LOTION FOR L/A BD/ 2WEEKS.
Discharge summary:
CHIEF COMPLAINT: A 57 year old female,house wife by occupation came with complaints of pain in abdomen since 2 months, iching all over the body since 1 month,generalized weakness , yellowish discoloration of sclera and skin and stools since 25 days.
HISTORY OF PRESENTING ILLNESS:
Patient was apparently asymptomatic 2months back then she developed
pain over the periumbilical region ,pricking type of pain ,non radiating,no aggrevating and relieving factors.
1 month back then she noticed yellowish discoloration of eyes and urine and went to hospital and on further evaluation she was diagnosed to have type 2 diabetes mellitus and was started tab.dapgliflozin 10mg in the morning and tab.sitagaliptin 50mg + t.metformin 500mg at night.
H/o occasional tingling and numbness of upper limb and lower limb.
No c/o polyphagia,polydypsia,nocturia.
Past history -
K/c/o diabetes mellitus 2months and on tab.dapgliflozin 10mg in the morning and tab.sitagaliptin 50mg + t.metformin 500mg at night.
In 2010, she had difficulty in breathing during winter season and monsoons (? Bronchial Asthma ) and used tab.deriphylline 450mg 1/2 tab PO/BD for 5-7days during the attacks along with inhaler ,presently she is not having any difficulty and not using.
Not a k/c/o HTN, Epilepsy, thyroid disorders,CVA.
Surgical history:
In 1996 diagnosed to have tumour of the uterus - hysterectomy done.
Personal history:
Normal - appetite
Adequate -sleep
Regular bowl movements
Normal bladder movements
No history of alcohol, smoking and chewing of tobacco .
FAMILY HISTORY:
No significant family history.
General examination:
Patient is conscious, coherent and cooperative.
Pallor present.
No clubbing, cyanosis, lymphadenopathy,odema.
Icterus - present
Vitals -
Bp - 110/70mm hg
Pr - 86bpm
Rr-16cpm
SYSTEMIC EXAMINATION:
CVS:
S1 and S2 heard.
No addded thrills or murmurs heard
RESPIRATORY SYSTEM:
Normal vesicular breath sounds heard.
Bilateral air entry present.
ABDOMEN:
INSPECTION:
shape of abdomen - schaphoid.
umbilicus -central
no sinuses
No scars
PALPATION:
Tenderness+ over right hypochondriac region
PERCUSSION:
No shifting dullness
AUSCULTATION:
Bowel sounds +
CNS:
Conscious and coherent.
Normal sensory and motor responses
COURSE IN HOSPITALS:
patient came with complaints of pain in abdomen since 2 months, iching all over the body since 1 month,generalized weakness , yellowish discoloration of sclera and skin and stools since 25 days,after doing all investigations and examination patient is diagnosed as Extrahepatic biliary obstruction secondary to head of pancreas mass
( Maglingnant ?) with ERCP + CBD stenting done on 24/7/23 with T2 DM and S/P EUS + FNAC done on 3/8/23 WITH ? BRONCHIAL ASTHMA ,Pruritus secondary to obstructive jaundice.
22/7/23:
Surgery refferal was taken I/v/o
Pain in abdomen since 2 months, yellowish discoloration since 2 months, itching all over body since 2 weeks
After examining patient they adviced for ERCP for pancreatic duct stenting with or without biopsy and to continue same treatment.
On 24/7/23
Patient was done to KHL for gastro opinion and was adviced for ERCP along with CBD stenting ,if possible biopsy from head of pancreas .
Procedure was done.
S/P: ERCP+ CBD STENTING DONE.
Biliary brushings were taken.

26/7/23:
Surgery referral was taken I/v/o pain and tenderness umbilical and right hypochondriac region and
After examining the patient,they advised
1.Inj magnex forte 1.5 mg IV/BD
2.Inj pcm 1gm IV/BD
3.Inj buscopan IM/STAT.
Surgical oncology opinion was taken on 26/7/23 has adviced to wait for cytology reports and repeat lft after 2 weeks to know the status of decompression and if the lft is improved and based on cytology report decision of surgery will be taken(whipples procedure).
and has adviced cect abdomen triple phase with pancreatic protocol to know if the mass is operable or not and location of mass(pancreatic head or mid CBD as reported in ercp) and previous cect films were of poor contrast.
29/7/23:
Gastroreferral taken today as advised for follow up after 5days by khl gastroenterologist they adviced USG abdomen and LFT.


3/8/23:
Patient has been taken to khl for EUS and FNAB.



5/8/23:
Derma refferal was taken I/v/o pruitits and has been advised to take
1.VENUSIA MAX LOTION FOR LA/BD/2 weeks.
PATIENT IS BEING DISCHARGED AT HEMODYNAMICALLY STABLE STATE
INVESTIGATIONS:
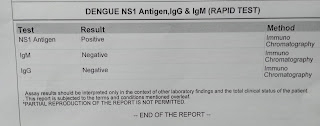
22/7/23
Serology -negative





Chest X ray:

ECG:

2D echo:

31/7/23
USG:

LFT:

Treatment:
1.TAB ZOFER 4 MG PI/TID
2 .TAB ULTRACET 1/2 TABLET PO/QID
3.TAB AVIL 25 MG 1/2 PO/QID
4.TAB PAN 40 MG PO/OD BBF
5.VENUSIA LOTION LA /BD/2 WEEKS
ADVICE AT DISCHARGE:
1.TAB ZOFER 4 MG PI/TID
2 .TAB ULTRACET 1/2 TABLET PO/QID
3.TAB AVIL 25 MG 1/2 PO/QID
4.TAB PAN 40 MG PO/OD BBF
5.VENUSIA LOTION LA /BD/2 WEEKS